




On a recent visit to Shenyang, located in the North-East of China, I met with Dr Baosen Zhou to discuss the endemic of Neurocysticercosis in this densely populated region. Neurocysticercosis (NCC) is the most common parasitic disease of the nervous system and is the main cause of acquired epilepsy in developing countries. It has also been a problem in industrialized countries because of the immigration of tapeworm carriers from areas of endemic disease.
Neurocysticercosis is usually acquired via fecal-oral contact with carriers of the adult tapeworm Taenia solium. This outcome would sometimes indicate the presence of a tapeworm carrier in the immediate environment (i.e, household or work) or by ingestion of contaminated food.
The biology of Neurocysticercosis
Neurocysticercosis is the result of accidental ingestion of eggs of Taenia solium (ie, pork tapeworm), usually due to contamination of food by people with taeniasis. T solium has a 2-host biologic cycle, with humans as the definitive hosts carrying the intestinal tapeworm, and pigs as the normal intermediate hosts harboring the larvae or cysticerci. This parasite has a head (scolex) with 4 suckers and a double crown of hooks, an unsegmented neck, and a large body with several hundreds of hermaphrodite proglottids.
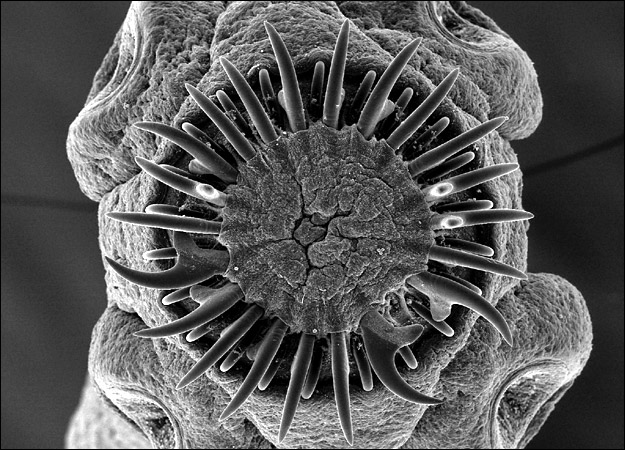
The pork tapeworm; image courtesy of Dennis Kunkel Microscopy, Inc.
Cysticerci are ingested by humans through poorly cooked infected pork. Cysts evaginate in the small intestine, attach to the wall by its suckers and hooks, and develop strobila or chains of proglottids. From the distal end of the strobila, fertile eggs are excreted into the gravid proglottids. Up to 60,000 eggs may be contained in a single proglottid.
Pigs ingest stool contaminated with Taenia eggs, the embryos actively cross the intestinal wall, get into the bloodstream, and are transported to most tissues, where they reside as cysticerci. Larvae are found most commonly in the central nervous system (CNS), but they can also be located in the eye, muscle, or subcutaneous tissues.
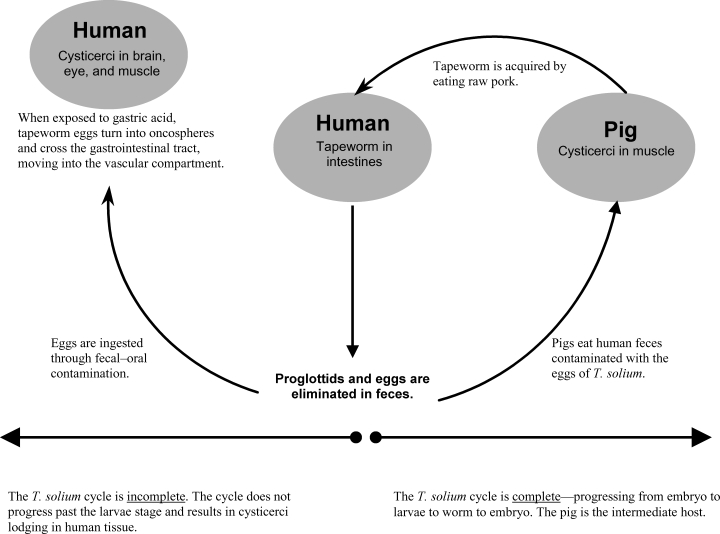
Life cycle of Taenia soliumLife cycle of Taenia solium; diagram from PMCID: PMC1176337
g
g
We asked Dr Zhou a few questions about this growing problem in Shenyang.
What has caused this problem in Shenyang?
“In Shenyang there are a lot of small vendors selling pork and other meat products, which are sometimes undercooked.These small fast-food outlets try to cook the food very fast in order to meet the demand and so worms and eggs may remain alive in any infected meat.
Poor hygiene with food handlers is also a big problem so cross-infection is common. Yet another problem is education, there are many people who are not aware of the dangers with infected meat. Most people believe parasitic worms reside only in the gut and are not aware of the potential to migrate to the brain, eyes and heart.”
What can be done?
“In the United Kingdom and the US, laws on feeding practices and the inspection of domestic food animals have largely eliminated tapeworms.
Avoiding raw meat and cooking meat well enough (to greater than 140 degrees F for 5 minutes) will prevent tapeworm infection. Freezing meats to -4 degrees F for 24 hours also kills tapeworm eggs. Good hygiene and hand washing after using the toilet will prevent self-infection in a person who is already infected with tapeworms.”
Why pork?
“Tapeworms are not restricted to pork only. Cattle usually carry Taenia saginata (T. saginata). Pigs carry Taenia solium (T. solium). Pork tapeworms, however, have a unique feature in being able to cross the intestinal wall and enter the vascular compartment where they can then migrate to other organs, including the brain. When a pork tapeworm infects the brain it is called neurocysticercosis.”
Potentially some people may be living with this parasitic worm but not have any severe manifesting symptoms. What other symptoms may give indication to a parasitic infection?
If the patient does not present with any serious clinical symptoms such as seizures, severe headaches or increased intracranial pressure then it may be difficult to detect. For example, if the worm has embedded itself in muscles of the leg then it may not have any major effect on that persons quality of life. On the other hand, if it were to enter the lymphatic circulation and block the lymph flow causing edema in the lower limbs then we would know to intervene. It is advised that people take the necessary precautions and prevent infection. It has been reported, however, that some patients feel increasingly lethargic once infected.
What precautions should people take?
People should:
- Wash hands before and after using the toilet or touching the area around the anus
- Wash hands before and after handling food, especially raw products
- Cook meat at a temperature greater than 140 degrees F for 5 minutes
- When storing meat in a freezer make sure it is below -4 degrees F
- If there is evidence of a white worm in your stool then book an appointment with your physician
Is Neurocysticercosis a problem in the rest of the world?
Most medical issues are not isolated. With trans-atlantic flights, an endemic in China is very much an endemic in any other part of the world. It’s not surprising then to discover that Neurocysticercosis is occurring more frequently in all industrialized cities. It is important to raise public awareness so that people will ensure they cook their meat thoroughly and store frozen meat in the appropriate conditions. People should also be very cautious about where they eat food, as poor hygiene from an already infected person is the key route of infection for developed countries.
g
g
Sources
- Gubbay AD, Brophy BP, Henley S, Sage M. Neurocysticercosis. J Clin Neurosci. Apr 1998;5(2):203-7. [Medline].
- Sinha S, Sharma BS. Neurocysticercosis: a review of current status and management. J Clin Neurosci. Jul 2009;16(7):867-76. [Medline].
- Del Brutto OH, Garcia E, Talamas O, Sotelo J. Sex-related severity of inflammation in parenchymal brain cysticercosis. Arch Intern Med. Mar 1988;148(3):544-6. [Medline].
- Gaffo AL, Guillen-Pinto D, Campos-Olazabal P, Burneo JG. [Cysticercosis as the main cause of partial seizures in children in Peru]. Rev Neurol. Nov 16-30 2004;39(10):924-6. [Medline].
- Bickerstaff ER, Cloake PC, Hughes B, Smith WT. The racemose form of cerebral cysticercosis. Brain. Mar 1952;75(1):1-18. [Medline].
- Del Brutto OH, Santibanez R, Noboa CA, Aguirre R, Diaz E, Alarcon TA. Epilepsy due to neurocysticercosis: analysis of 203 patients. Neurology. Feb 1992;42(2):389-92. [Medline].